June’s Tip

Orthodontics From Inception to Retention
By Milton Pedrazzi, IBO Diplomate, IAO Certified Instructor
June 2026
2018 Valley Oak Road
Pleasanton, CA 94588
United States
DIAGNOSIS of the CASE
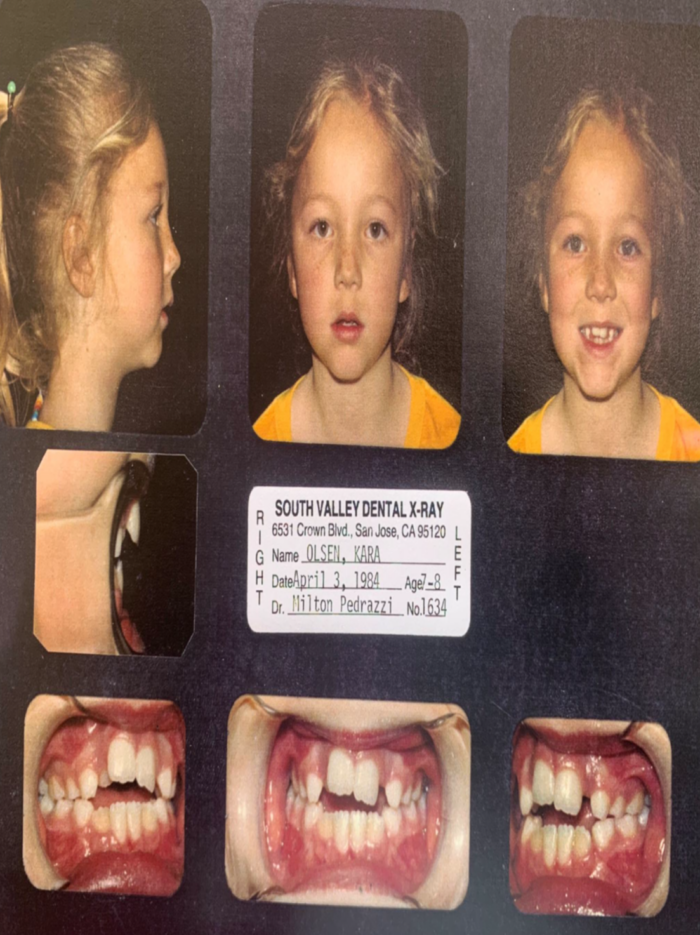
1. Kara’s case had an open bite plus a tongue thrust and a thumb sucking habit. I tested her for the ability to breathe through her nose which she was able to do even though her cephalogram appeared to reveal a large mass of adenoidal tissue. She had an extremely crowded dentition and an open bite.
2. Kara was 7 years and 8 months old when beginning records were taken.
3. Both the upper and lower arches were extremely crowded with a canted occlusal plane on her upper arch.
4. Her vault is not deep indicating she has some tongue pressure in her vault when swallowing.
5. She has a mesiodens high in her alveolus.
6. The apparent tired look in her eyes is not uncommon in patients with high mandibular angles who are mouth breathers.
7. Noteworthy in her cephalogram analysis is a high SnGoMe angle of 45° and a Type I symphysis with a nasopharyngeal airway that may be partially restricted.
8. Even though her arch space is extremely lacking, due to the consideration for facial esthetics plus the goal of a full smile it is desirable to do this case non-extraction. Bite wing x-ray films indicate that the permanent bicuspids are not excessively large.
9. Her lower cuspids are completely blocked out on both sides.
10. Her upper and lower dentition is extremely crowded.
11. She has a weak Class I molar relationship.
12. No crossbites.
13. She has 12 permanent teeth either fully erupted or partially erupted and 10 fully erupted primary teeth.
14. Her overjet is +6 to +7 millimeters.
15. Her cephalometric analysis reveals a clockwise growth pattern with a mandible that is too short to provide a nice profile in a finished result.
TREATMENT
1. Treatment is designed to rotate the Premaxilla downward to correct the open bite and the canted occlusion and produce a pleasing smile at the end of treatment.
2. An increase in Sagittal arch length is needed to make room for her teeth on both the upper and lower arch.
3. To accomplish this task a Bionator type appliance is indicated. This appliance is of special design. The design is to aid in closing the bite and lengthening the upper lip and lower lip while advancing the mandible. To accomplish this task a modification of the Bionator is indicated as it is used to lengthen the Upper Lip while advancing the mandible.
4. Labial pads are placed on the both the upper arch and lower arch portion of the Bionator to encourage arch development in these areas.
5. The goals of treatment are as follows:
a. Rotate the premaxilla downward and forward.
b. Torque the crowns of the lower anterior teeth labially.
c. Reduce the lip pressure on the lower anterior segment and the Upper anterior segment.
d. Control the tongue thrust habit.
e. Gain Upper arch length by creating a strong Class I molar relationship.
f. Gain lower arch length by tipping the lower anterior teeth labially.
g. Gain bony growth in the Sagittal direction by decreasing lip pressure from the upper and lower anterior teeth.
h. Increase the length of the Upper Lip as the maxilla is rotated downward.
i. Finish Kara’s case with a Class I molar and cuspid dental occlusion with midlines on and a pleasing smile and good dental function.
TREATMENT SUMMARY:
Treatment began by placing a bite closing Bionator on 1/12/85. This Bionator was modified with methyl methacrylate lip pads in front of both the upper and lower anterior teeth. The design was meant to encourage appositional growth on the anterior part of the maxilla and mandible and to encourage lengthening the upper lip. By 04/01/85 her bite had closed down considerably and the overbite was near edge to edge. The overbite remained with some improvement. The lip position had also improved. The appliance was lost by the patient after 4 months. A new appliance of the same design was made on 5/6/85. Kara wore this appliance for another 2 years. By 12/5/85 the lip position appeared normal. On 5/19/86 the lower arch space was measured and the lower teeth were within 3 millimeters of having sufficient space to be accommodated by the mandible.
On 5/21/87 the lower first molars were banded and a slightly oversized lingual arch was placed to gain arch length for the lower teeth. On 10/23/87 the mesiodens was removed by an oral surgeon.
On 12/02/87 the upper and lower arches were banded and bracketed as by now sufficient arch length had been gained to accommodate all the teeth. During treatment midline cross elastics were used to correct the midline. Pericoronal tissue was removed from tooth #18 and tooth #31 before they erupted in too high a posture. Bracketing these lower 2nd molars early lessens the likelihood of opening the bite when going through the wire changes. For the next 1 1/2 years wire changes were made as orthodontic treatment went forward. More midline correction was needed so on 3/20/89 the upper wire was placed with the midline of the wire in the distal portion of the bracket on tooth #8. On 5/23/89 more expansion was needed from cuspid to cuspid in the upper arch so an .018 Australian wire was placed upper cuspid to upper cuspid as a piggy back sectional wire. The tongue thrust habit persisted so a tongue thrust appliance was delivered on 11/12/89. A step out bend was placed on the upper first molars on 3/12/90 to gain a better molar relationship. Swallowing exercises were started on 9/20/90 in addition to the tongue thrust appliance. On 11/13/90 the arch wires were bent to encourage bite closure. On 2/05/91 Box elastics were placed on the anterior teeth to close the bite. These mechanisms served to close the bite and the bands and brackets were removed on 3/18/91. On 5/01/91 a lower fixed retainer was placed from lower 1st bicuspid to 1st bicuspid.
RESULTS:
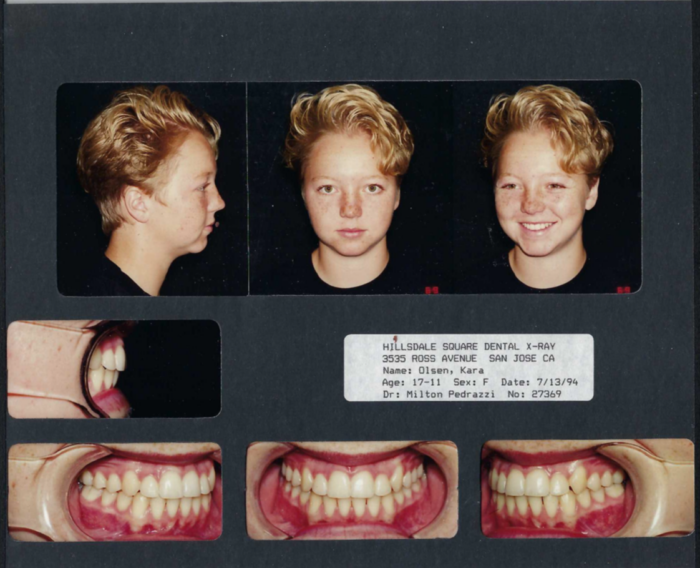
Kara conquered her tongue thrust habit. She now has a Class I molar and cuspid dental occlusion and a pleasing smile with a nice profile due in large part that we were able to accomplish this case without bicuspid extractions. She now has complete lip competence. Her occlusion is good and interestingly she has gone from a Type I symphysis to a Type II symphysis with an increase in her mandibular body length from 60 millimeters to 70 millimeters. It appears that there was appositional bony growth on the labial aspects of the maxilla and mandible.
Although this case worked out well, today I would correct the tongue thrust and swallowing habit in the beginning of treatment. Teaching the patient the correct method and mechanics of the swallow should be addressed at the beginning of treatment as eliminating a tongue thrust or a thumb sucking habit early simplifies future orthodontic treatment.

We learn by our experiences.
The Orthodontic case finish should be visualized at the beginning of orthodontic treatment. The diagnosis from the records with particular emphasis on the Lateral Head Film angles and linear measurements cannot be overemphasized and will help to visualize the patient’s final orthodontic result. This understanding plus gnathological consideration of the TMJ’s immediate and long term health and incorporating those needs in the original treatment plan should result in a successful result for the patient. Gnathological and muscle function consideration aids greatly in the retention design and future maintenance of that result.
Milton E. Pedrazzi DDS